Shot, Then Shut Out
Chicago’s most crime-ridden neighborhoods have no access to trauma care.
Rebecca Burns
The nation finally took notice of Chicago’s epidemic of gun violence after 15-year-old Hadiya Pendleton was fatally shot January 29. Pendleton was the city’s 42nd victim that month, but her appearance at President Obama’s inauguration just weeks before pushed her death to the center of a national conversation on gun control. Since 2008, more young people have been killed in Chicago than in any other American city — a statistic that has sent city officials in search of solutions to plug loopholes in gun policy and crack down on gang violence.
But Veronica Morris-Moore, 20, a community organizer from Chicago’s Woodlawn neighborhood, believes politicians are looking for solutions in the wrong places. “If they’re not going to talk about the economic violence that causes gun violence, then I’m not interested in the conversation,” she says.
Left out of the gun-control debate, Morris-Moore says, are the poverty and lack of services that plague neighborhoods with high rates of gun violence — including what she calls a “trauma care desert” for gunshot victims on Chicago’s South Side.
Dedicated trauma care units, which are staffed to provide around-the-clock specialty care for victims of shootings, car crashes and other calamities, give victims better odds of survival. But in Chicago and other urban areas across the nation, they’re increasingly in short supply.
The University of Chicago’s ivy-covered campus, nestled amid some of the city’s poorest neighborhoods, hosts the only Level I trauma center on the South Side. However, the center is open only to children age 16 and younger. Adults who sustain critical injuries in the area must be transported to other hospitals on the North or West Sides of the city.
That’s exactly what happened in 2010 when 18-year-old community activist Damian Turner was gunned down in a drive-by shooting a mere four blocks away from the University of Chicago Medical Center (UCMC). Ambulance drivers were required to rush Turner to the nearest trauma center nine miles away, and he died shortly after arriving. His death sparked a push by the activist group he founded, Fearless Leading by the Youth (FLY), to pressure UCMC to raise the age limit of its trauma center to 21.
When UCMC’s trauma center first opened in 1986, it operated an adult trauma care unit, but decided to close it after two years due to annual losses of $2 million. In response to the FLY campaign, John Easton, a UCMC spokesperson, told the New York Times in 2010 that the adult care unit was overburdened: “We drew the entire South Side,” he said. “That became overwhelming. It put an enormous strain on the hospital.”
The shuttering of UCMC’s trauma center was a forerunner of a nationwide wave of such closures. In 1990, the United States had 1,125 trauma centers; today there are 282, according to a list maintained by the Trauma Center Association of America. Dedicated trauma care, a paradigm of emergency medicine pioneered in Chicago in the 1960s, is costly to provide and receives little federal or state funding.
By 2007, 24 percent of Americans had to travel further to the nearest trauma center than they had in 2001, according to a 2011 Health Affairs study by researchers Renee Yuen-Jan Hsia and Yu-Chu Shen. Communities with large numbers of African American, poor or uninsured residents were disproportionately impacted, the study notes. An October 2011 analysis by the NPR affiliate WBEZ concluded that travel times for patients on Chicago’s Southeast Side from the scene of an emergency to trauma centers are 50 percent longer, on average, than those of other city residents.
A UCMC position paper on the issue asserts that singling out the dearth of trauma centers is misleading, because it is only “part of a much larger issue of unmet health needs.” It also references a 2010 national study that found — contrary to common assumptions — that longer ambulance run times do not increase mortality.
However, Marie Crandall, an associate professor of surgery at Northwestern University who is studying the relationship between survival rates and proximity to trauma centers, says that Chicago’s high rates of stabbings and gunshot wounds, which come with increased risks such as hemorrhaging, may result in different outcomes than those found in nationwide studies.
The debate over ambulance run times may mask a bigger picture. Overall, minority and uninsured patients are more likely to die following traumatic injuries than white and insured ones, according to a 2008 study in the journal Archives of Surgery. Racial disparities in access to healthcare are among the factors that have left life expectancies for African Americans lagging consistently behind those of their white counterparts—a 2012 study found that white men still outlive African-American men by an average of five years, and white women outlive their African-American counterparts by four years. High-quality care for trauma victims, who are frequently poor and uninsured, could help ease this gap — but its delivery tends to mirror broader racial inequities.
The cascade of trauma center closures around the country epitomizes the challenges to combating healthcare inequities in a for-profit system. The Emergency Medical Treatment and Labor Act (EMTALA), passed by Congress in 1986, is supposed to guarantee patients’ access to emergency care regardless of their ability to pay. The law outlawed “patient-dumping,” the practice of diverting the poor and uninsured to other facilities, and prohibited hospitals from transferring patients elsewhere unless they required treatment that couldn’t be provided onsite. But these changes merely produced a new form of patient-dumping: Since trauma centers, like burn units and other specialized services, were required under EMTALA to accept patients if requested, researchers have noted an uptick in transfers of poor and uninsured patients to trauma units, even when such moves are medically unnecessary.
In the absence of federal or state regulations mandating the availability of trauma care, hospitals in high poverty areas have found that simply closing their trauma units improves their bottom line. (Trauma centers may be more profitable in suburban areas where trauma density is typically lower, and patients more likely to have private insurance. Since 2009 HCA Holdings, the nation’s largest for-profit hospital chain, has opened dozens of trauma centers in communities such as Orange Park, Fla.)
One solution, advocated by the nonprofit Trauma Center Association of America, is to increase federal funding for planning and implementation of improved regional trauma care networks.
Morris-Moore acknowledges that the University of Chicago Medical Center can’t fix the problem on its own, but says that its policies are “unfair to the community that they occupy.” Chicago health activists also believe that the medical center is attempting to hide a harmful agenda behind a charitable veneer.
The University of Chicago and other nonprofit hospitals receive local, state and federal funding in the form of tax breaks for providing “charity care.” In theory, such care should be a key component of the healthcare safety net for poor and uninsured patients, especially in areas such as trauma care. But a 2009 study by the Center for Tax and Budget Accountability estimates that the University of Chicago receives annual tax breaks worth $59 million, more than five times what it spends on the provision of free or reduced-cost treatment. (UCMC asserts that it spends $200 million annually on services to the poor, including not only charity care but losses from unpaid bills and Medicare and Medicaid patients).
In 2009, the American College of Emergency Physicians warned that a proposed reduction in the number of emergency beds at UCMC was “dangerously close to patient-dumping.” Though hospital administrators ultimately canceled the change, critics say that the university is attempting to cherry-pick wealthy patients by reducing emergency care while expanding more lucrative elective procedures. In addition to closing its adult trauma unit, the medical center initiated a program aimed at redirecting non-emergency cases to neighborhood clinics in 2005. The Urban Health Initiative launched by First Lady Michelle Obama while an executive at the medical center has been assailed by some practitioners as a dangerous precedent for wealthy hospitals serving poor communities. UCMC notes in its position paper that its 537-bed facility is overcrowded and “cannot by itself solve all the problems of an area [of Chicago] that has lost more than 2,000 hospital beds in recent decades.”
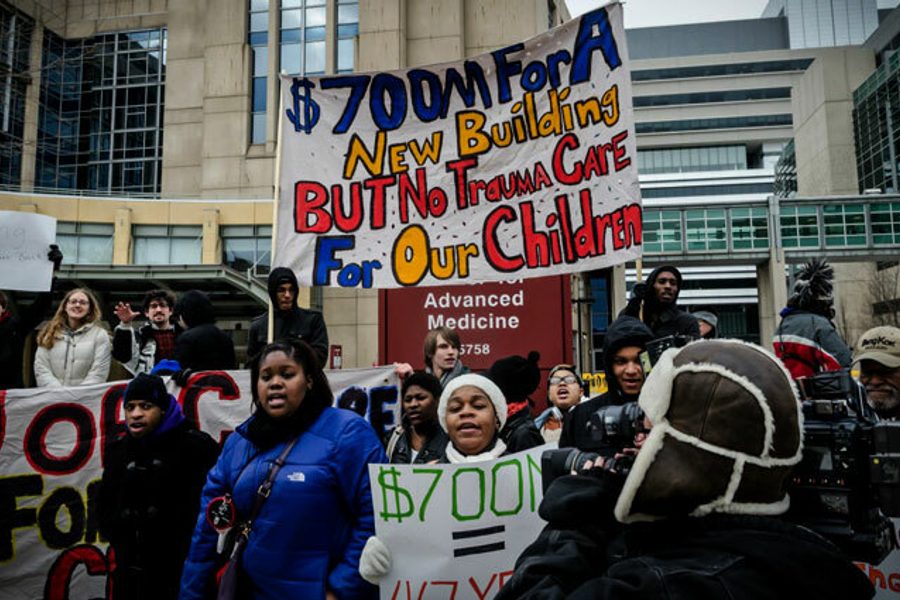
Most controversial is the $700 million that the university has put toward the Center for Care and Discovery, a new building devoted to specialty care. On January 27, about 50 demonstrators from FLY staged a sit-in during an invitation-only tour of the building, chanting, “How can you ignore? We’re dying at your door!” Campus police quickly arrived on scene and expelled the group using what Morris-Moore describes as excessive force. She had planned on staying and risking arrest after others dispersed, but says she was kneed in the back by a campus police officer and dragged off the premises. Four demonstrators, including one man taking video of the event, were arrested and charged with criminal trespassing. Following subsequent demonstrations in support of the arrestees, they were offered a plea deal and received supervision in place of fines or jail time.
In a statement following the protest, the university said that campus police had initiated a review of the incident, per normal procedures. University Provost Thomas Rosenbaum also announced a series of dialogues on campus protest, policing and community relations.
For Morris-Moore, the rough treatment was emblematic of the way that black youth in the area are both excluded and criminalized. “The message I got that day is the same message I’ve been getting in more subtle ways for a long time: The University of Chicago doesn’t care about these youth,” she says.
Alondra Nelson, an associate professor of sociology at Columbia University, notes that the trauma center campaign taps into a long history of black community organizing for access to healthcare. Initiatives like the Black Hospital Movement and the Black Panthers’ free clinics sought to highlight and compensate for African Americans’ exclusion from healthcare facilities and medical schools, which, Nelson says, “have been some of the key ways that racial discrimination has proceeded in American society.”
She believes that tradition is still vital today. “Medical discrimination has become more subtle,” she notes, “but in some ways that makes it more insidious.”

Rebecca Burns is an award-winning investigative reporter whose work has appeared in Business Insider, the Chicago Reader, the Intercept, ProPublica Illinois and other outlets.